18ECO124T - HUMAN ASSIST DEVICES UNIT 4 & 5 - 12M
12M:
SET 1:
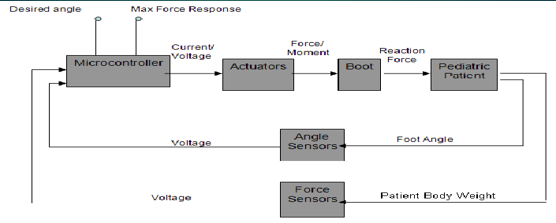
Write in detail about the pediatric orthosis with a diagram
Pediatric orthosis:
There are several respects in which a child's orthotic requirements differ from those of an adult and these may extend beyond treatment of the obvious abnormality.
Accordingly, before considering specific hardware and research activities, the criteria affecting the performance of an orthosis will be discussed.
A child is a particularly dynamic person in terms both of his activity and of his developing personality.
It is important that there is a full appreciation of these factors so that prescription of an orthosis can be made sympathetically and in harmony with his development
Human factors:
Many physical and emotional factors can affect the success of an orthosis
Physical factors can be considered under the headings of deformity, growth and activity
Deformity:
Frequently an orthosis is fitted to prevent the development of a deformity, particularly during periods of rapid growth
For instance, knee and hip flexion contractures may develop rapidly if the child is wheelchair-bound but may be prevented if he is provided with an orthosis which permits an upright stance and mobility for at least a part of each day
Growth:
The prime reason for including adjustability within the orthosis is to accommodate the growth, although at certain sites growth cannot be handled in this way
A weight penalty, from the adjustable components is inevitable and this option should be balanced against the replacement of certain parts
Activity level:
A child’s natural desire to participate in games and to move from one place to another rapidly, provided there is motivation for doing so, as exemplified by the able-bodied child who runs, hops, skips and jumps whilst out for a 'walk'.
As far as possible, the orthosis should permit the handicapped child to achieve the highest possible level of activity compatible with his disability and it should not represent an additional handicap in itself
Change of attitude/location:
An orthosis should be unobtrusive both in appearance and in its effect on daily living activities
Ideally a child should be able to stand up/ sit down, transfer to/from a wheelchair or road vehicle, go to the toilet, attend school, without having to remove his orthosis
The emotional and physical effort of such maneuvers should be minimal if the child is going to achieve his maximum potential
Elaborate in detail about the Intermittent positive pressure breathing (IPPB) assistance for lungs
Intermittent Positive Pressure breathing (IPPB) is an assisted breathing technique used to provide short term or intermittent mechanical ventilation via mouthpiece or mask for the purpose of augmenting lung expansion and delivering aerosol medication
IPPB is inspiration using a non-invasive ventilator such as the Bird and Bennett with pressure boost
The Bird Mark 7 ventilator is a pressure cycled device convenient to use for providing IPPB
Indication for IPPB:
To improve lung expansion
To clear secretions
To relieve bronchospasm
Procedure for IPPB:
Explain procedure to patient
Attach circuit tubing, valve line and nebulizer tubing to IPPB machine
Block the mouthpiece with sterile gauze
Aseptically prepare medication and insert in the IPPB
Purse lips around mouthpiece
Breathe through the mouth only
Inspire slowly and deeply
After patient is comfortable, treatment can begin
Set sensitivity control according to patient
Adjust inspiratory pressure accordingly
Adjust nebulizer controls accordingly
Monitor the patient throughout
When treatment is complete, detach circuit from IPPB machine
Frequency for use of IPPB:
Critical care: every 1 to 6 hrs for IPPB is tolerated. IPPB order should be re-evaluated at least every 24 hours
Acute/ home care patients: common strategies for IPPB vary from b.i.d to q.i.d
For acute care patients: order should be re-evaluated at least every 72 hrs
Home care patients: should be re-evaluated periodically
Contra indication of IPPB:
Hiccups
Nausea
Hemodynamic instability
Recent facial, oral or skull surgery
Recent esophageal surgery
Increased intracranial pressure
Tracheoesophageal fistula
Limitations:
All the effects are short lived, only lasting for an hour after treatment
Based on available literature, MDI or compressor driven nebulizers should be considered as best choice, not IPPB
The dose of IPPB is tenfold compared to MDIs
Efficacy of the device is technique dependent
SET 2:
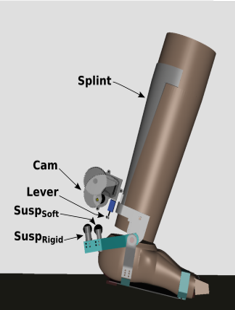
Explain briefly about the Foot Orthosis with a neat Diagram
Foot orthosis is a medical device employed to support and align the foot, in order to prevent or correct foot deformities and to improve the function of foot
Foot orthoses aim at
correcting static and dynamic disorders of the foot
Relieving painful overloaded areas by distributing bearing forces
Protecting and preventing trophic risks
Accommodating fixed lesions
Stimulating anatomic parts of the foot
Foot orthosis is the fundamental component of any lower limb orthotic system
Functions:
Reduce stress and strain on ankle, foot, knee, hip and spine
Correct abnormal foot position
Support arches of foot
Equalize limb length discrepancies
Protect the foot from injurious stimuli
Foot orthosis includes:
Foot wear (shoe, chappal, sandal)
Footwear modifications (external modification and internal modification)
Shoe inserts (rigid, semi rigid, soft)
Commonly used in:
Heel pain
Toe pain
Club foot
Insensitive foot
Limb length discrepancy
Different types of foot orthosis:
Corrective orthoses
Accommodation orthoses
Stimulatory orthoses
Preventive orthoses
Types of materials used:
Leather and leatherwork derived from animal hides
Glues
Materials composing orthotic inserts
Types of lower limb orthosis:
Foot Orthosis (FO)
Ankle Foot Orthosis (AFO)
Knee Ankle Foot Orthosis (KAFO)
Hip Knee Ankle Foot Orthosis (HKAFO)
HKAFO with spinal support
Knee orthosis:
Enclose the knee joint extending as far as mid-thigh and mid-calf
Types:
Soft
Rigid
AFO:
Most commonly used orthosis
AKA below knee brace, below knee iron, short caliper
Frequently described for patients with gait deviations resulting muscle dysfunction around ankle and foot
KAFO:
Are for individuals who have significant weakness or deformity in the lower extremities
Are made from metal and leather
HKAFO:
Combine componentry at the hip and pelvis as well as the knee and foot and ankle
Usually prescribed for:
Paraplegia
Paraparesis
Paralysis
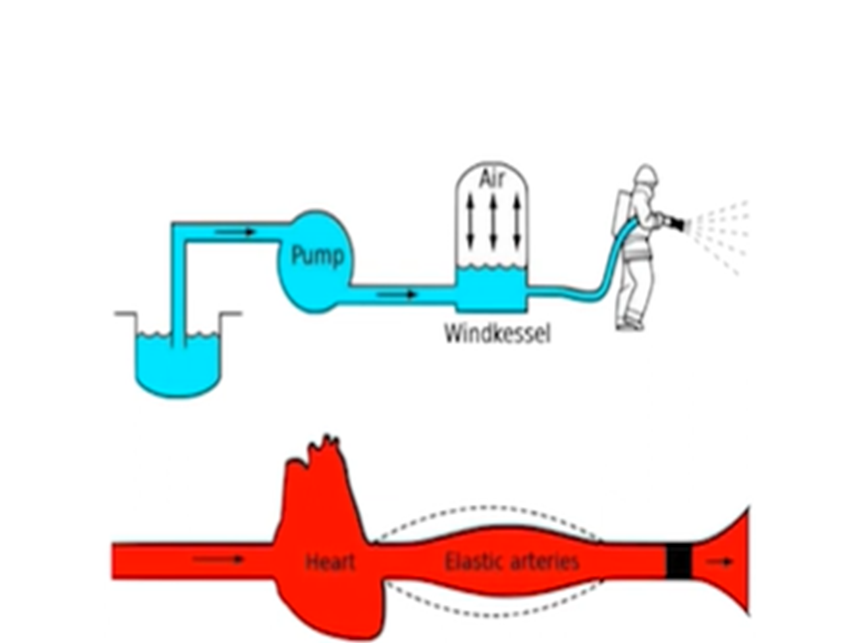
Summarize the working of Intra-Aortic Balloon Pump with a neat diagram.
Intra-aortic balloon pump:
Intra-aortic balloon pump (IABP) remains the most widely used circulatory assist device in critically ill patients with heart disease
The primary goal of IABP is to improve the ventricular performance of the failing heart by facilitating an increase in myocardial oxygen supply and a decrease in myocardial oxygen demand
The IABP catheter is inserted percutaneously into the femoral artery through an introducer sheath using the modified Seldinger technique
History:
Kantrowitz described augmentation of coronary blood flow in 1952
In 1958, Harken suggested diastolic augmentation
4 years later, Moulopoulos and colleagues developed an experimental prototype of an IABP
Principles of Intra-Aortic Balloon Pump (IABP)
Mechanical Assistance: The IABP is a mechanical device designed to help the heart pump blood; It is inserted into the aorta
Counterpulsation: The principle of counterpulsation is central to the IABP's function. The balloon inflates and deflates in sync with the cardiac cycle
Inflation and Deflation Timing:
- Diastole (Inflation): During diastole, when the heart is at rest, the balloon inflates
- Systole (Deflation): Just before systole, the balloon deflates
Helium Gas: Helium is used to inflate and deflate the balloon
Synchronization with ECG: The IABP is synchronized with the patient's electrocardiogram (ECG) to ensure precise timing of inflation and deflation.
Physiological effects:
Enhancement of LV function
Improve RV function
Reduces RV afterload
Reduction in LA and pulmonary vascular pressures
The magnitude of these effects depends upon:
Balloon volume
Heart rate
Aortic compliance
Indications for IABP:
Cardiogenic shock
In association with CABG
In association with nonsurgical revascularization
Stabilization of cardiac transplant recipient before insertion of VAD
Problems Associated with Intra-Aortic Balloon Pump (IABP)
Vascular Complications
Thrombosis and Embolism
Balloon Rupture
Infection Risk
Malposition
Mechanical Failure
Comments
Post a Comment